HFA Development
Development of HFA
The following is a dot point summary of the development of HFA (Homœopathic Facial Analysis). HFA was developed between 1999 and 2021 by Grant Bentley – Principal of the Victorian College of Classical Homœopathy (VCCH). It is practiced around the world and taught from VCCH through online training.
History of the miasmatic project
- In 1999 VCCH undertook a project to determine what a miasm is and how to use it/them effectively in the clinic
- The foundation was the assumption that Hahnemann’s model of psora, sycosis and syphilis was valid in some way. The aim was to test the validity via the clinic. Could there by some systematic way to use Hahnemann’s miasmatic model to improve results?
- It was understood that the word “miasm” meant many different things to many different practitioners/methods
- However as Hahnemann’s tri-miasmatic model was the foundation of the project it seemed reasonable to keep the same terminology so the word “miasm” was still used
- Over the years as the facial analysis method validated (through the clinic) the existence of miasms. The understanding of what a miasm is began to change
Facial features and starting remedies
- There were references to facial features and their affinity to miasms in Homœopathic literature (Allen, Roberts, Foubister)
- Patients in the clinic who had responded well to miasmatically “known” remedies such as Sulphur (psora), Thuja (sycosis) and Mercury (syphilis) were photographed and their features compared
- Similarities were noted and further patients were analysed to determine if they too would respond to a polychrest known to be relevant to one of these three miasms
- About 50 features were noted and classified over a two year period
- The concept of hypo (psora), hyper (sycosis) and dys (syphilis) was used to understand the relationship between features and their primary miasm
- Hypo related to the concept of small or sloping, hyper to large, round and straight and dys to crooked, sharp or inward
- These same structural shapes were represented in facial features
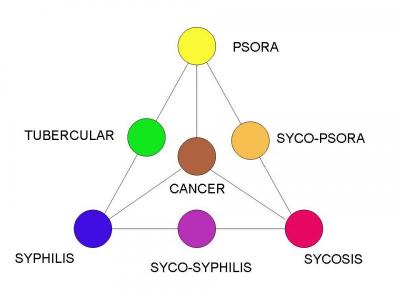
- It was considered that if it was true that there was a tubercular miasm (psora and syphilis combined in equal strength) and a cancer miasm (psora, sycosis and syphilis combined in equal strength) then there must be two other miasms
How many miasms?
- It was reasonable to accept that after 150 years of homœopathic theory the concept of a tubercular miasm would be true – the same could be said of the cancer miasm
- This deduction was based on the understanding that of the three primary miasms, if two of these could join (eg tubercular) mathematically there must be a total of three duo miasms and the one trio miasm
- This was deduced by using the model of dissimilar diseases – where two dissimilar diseases of equal strength can join to form a new disease.
- This hypothesis explained the existence of the tubercular and the cancer miasm
- If psora joined with sycosis then a miasm called syco-psora would exist
- If sycosis joined with syphilis then a miasm called syco-syphilis would exist
- This meant there could only be seven miasms – that is including the original three and all their possible combinations - only seven miasms could exist
- We understood that because the three primary miasms were the basis of the model the other four miasms were all that could exist as well as the base three
- So the tubercular miasm couldn’t join with the syco-psoric miasm because in essence this would mean one part psora and one part syphilis combining with one part sycosis and one part psora. In this example psora is twice as strong as either the syphilis or the sycosis making psora dominant in the patient
- A triangle was designed to visually represent this model
Hahnemann’s laws and dominance
- As more features were tested we came to see that most patients had features from all three primary miasms
- We knew that everyone couldn’t belong to the cancer miasm so examined the model again
- We focused on the laws as laid out by Hahnemann – a stronger dissimiliar disease would prevent the action of the weaker disease
- This concept was applied to the facial features of all patients presenting with chronic disease – now we call this “dominance”
- Phosphorus was used as a representation of the tubercular miasm
- Arsenicum was used as a representation of the cancer miasm
- Features of patients responding well to these remedies were examined
- Phosphorus patients had equal amounts of psoric and syphilitic features (as determined from the three primary miasms) that were dominant over any sycotic features
- Arsenicum patients had equal amounts of psoric, sycotic and syphilitic features
- It was deduced that the concept of dissimilars was as relevant to miasms as to diseases
- This was a revolutionary part of our understanding to all aspects of the model – from the dominance of facial features, to the dominance of one miasm over another to the dominance of a remedy over a disease. We began to understand that anything stronger in nature will overpower anything else that is weaker – Hahnemann had said so but the application of this idea had been limited to diseases and medicines only
- We spent some time determining what “equal” meant and decided by experiment that a factor of one feature ahead or behind the dominant miasmatic features still rated as equal
- For example 5 parts psora plus 6 parts syphilis is still tubercular even though the syphilis is one part greater – the ratio of 5 to 6 being close to equal
- However if a patient presented with 5 parts psora and 7 parts syphilis the syphilis was determined to be dominant over the psora making the patient syphilitic – the ratio of 7 to 5 showing a distinctive dominance
Allocating more remedies
- Although there are minor references to a syco-psoric miasm and a syco-syphilitic miasm no remedies are universally accepted as belonging to them
- Polychrests were examined to determine which ones could have equal amounts of psora and sycosis
- Nat Mur was classified as syco-psoric and clinically proven the same
- Lachesis was classified as syco-syphilitic and clinically proven the same
- This meant that a patient with equal amounts of two of the three primary miasms showing in their facial features responded very well to a remedy from the miasmatic group which consisted only of remedies showing equal amounts of the two miasms in them also – there was a match of the energy of the patient to the energy of the remedy
- We now had a rudimentary working model to allow for miasmatic analysis
- Remedies were categorised to their most obvious miasmatic classification through the study of materia medica, clinical outcomes and similarity to clinically proven remedies within a miasm. In summary remedies were examined via one, two or all three of the following -
Ø They had worked very successfully with chronic illness in a patient and the facial features determined the dominant miasm of both the patient and therefore the remedy
Ø Some remedies were classified by examination of the materia medica in an attempt to determine the dominance of each of the three primary miasms within a specific remedy – in most cases these remedies later showed clinically to be miasmatically correct
Ø A remedy was so similar in its presentation and dominance to another known miasmatic polychrest, that it was grouped with that miasm and then verified through the clinic (eg Hyoscyamus and Stramonium being so similar to Belladonna were classified as syco-syphilitic and subsequently worked successfully on patients whose features showed they belonged to the same miasm as the remedy)
- Faces were analysed and remedies chosen for those cases that matched both the totality of the case and the miasm of the patient (as determined by their facial analysis only)
The role of pathology in miasmatic classification
- Pathology alone was quickly rejected as a classifier of any of the seven miasms because each of the seven main polychrests had pathologies traditionally belonging to all of the three primary miasms – pathology wasn’t a truly distinguishing aspect of which miasm belonged to which remedy – only an outcome of a disordered miasm
- Each miasmatic group was renamed to break the mindset that a miasm and a specific pathology were mutually exclusive
- Psora became yellow, sycosis red, syphilis blue, syco-psora orange, syco-syphilis purple and cancer brown
Could a miasm change?
It was obvious that if features could determine a miasm then a miasm must be genetic*; existing at a deep cellular or sub-cellular level and not removable. Current patients provided photos of themselves when younger to determine what changes had occurred with their features over the years. There were difficulties because the older photos did not meet the current criteria for good quality images (easy to measure on a front and side angle) however enough information was present to determine the following –
- Where a patient was dominant in one miasm during their younger days the same dominance existed now
- In general older patients have more miasmatically classifiable features than younger patients but the dominance remained the same – on average young children have 6-10 features that can be determined miasmatically, adults 10-16 and older people 16+ (though individuals within these age groups can still vary widely in the amount of classifiable features) - the number of features makes no difference to the outcome – as we are only trying to determine the dominant miasm by the analysis of all the presenting features
By 2006 we understood that miasms were
- Genetic*
- Immovable
- Remained the same for life
- Could be determined by using facial features for analysis
- Could be calmed by a correct remedy
- Meaningful and useful to the patient on many levels – as well as being a force behind chronic disease
- The underlying drive to a patient’s personality type, how they reacted under moments of stress and which traits they had that helped them to manage better in their lives
- Clinically indispensable as a form of diagnosis when choosing a remedy or remedies for chronic illness
*By 2007 the concept of a miasm being solely genetic was reinterpreted as a miasm being a stress response – including the immune system, the nervous system, emotional responses and facial structure.
Homœopathy as an energy model
The HFA method led to a successful and reproducible clinical method using miasmatic understanding when choosing remedies for chronic disease. It also led to many questions about what Homœopathy was showing us about our natural world and our place as humans within that world. Was a miasm a good or a bad thing? Was the remedy working on a material level or an energetic level? What was the purpose of a miasm?
Discussions with students and colleagues led to the idea of a miasm as an energetic force that dictated the stress response of a patient. The seven groups had been renamed as colours once the link with disease was broken but the understanding of a specific energy force being responsible for the shape or size of a facial feature was a new idea. Psora became outward motion, Sycosis circular motion and Syphilis inward motion.
The qualities and traits of patients within the same miasm had some clear similarities. Many of these traits were positive and examination of these traits led to the idea and development of traditional roles. Within a short period of time an investigation of the relationship between a miasm (survival instinct) and epidemics uncovered the relationship between time and these energetic forces. Not only did the face uncover a way to use miasms as a clinical tool but they had also uncovered an understanding of Homœopathy that explained human behavior in stressful conditions and the relationship between Homœopathy, universal forces, time and social evolution. In 2008 Soul & Survival was written to explain these ideas.
Clinically the more we investigated the relationship between the patient and their energy levels, their energy balance (or usually imbalance) and the use of the Homœopathic remedy as an energy infusion the clearer the model became.
The origin of a miasm
The final question – where does the miasm come from? Why is a person born with the one particular miasm? This question is yet to be fully answered but there are some embryonic ideas about the relationship between the dominant parent and their personal dominant stress at the time of conception which may prove to be an explanation.
We do know that the miasm (survival instinct) is both a positive and a negative part of every person and that it can be used to select remedies that act at a deep level. We know that Homœopathy is the doorway to the energetic world and that through Homœopathy we can understand that world more fully.
- Log in to post comments